
Nandrolone (Deca Durabolin) has long held a controversial position in medical research and treatment for muscle health, especially regarding age-related muscle wasting. As one of the most well-known anabolic steroids, it’s essential to parse apart hype from evidence, especially when exploring its use in conditions like sarcopenia—the progressive loss of muscle mass that accompanies aging. This comprehensive review examines the clinical role, effectiveness, mechanisms, human evidence, and safety of Nandrolone in the context of muscle atrophy associated with aging and chronic disease.
Understanding Nandrolone Decanoate
Nandrolone decanoate, under the brand name Deca Durabolin, is a synthetic anabolic androgenic steroid (AAS) derived from testosterone. Originally developed for medical use to treat muscle wasting diseases, anemia, and osteoporosis, Nandrolone’s potent anabolic properties make it distinct from testosterone:
- Stronger anabolic effects: Promotes muscle protein synthesis more than testosterone
- Milder androgenic profile: Fewer masculinizing side effects
- Long-acting formulation: Administered by intramuscular injection, steadily releasing over 2–3 weeks
These pharmacological advantages underlie its historical use in treating various forms of muscle insufficiency, including those found in elderly populations.
Why Do We Lose Muscle as We Age?
Sarcopenia refers to the age-related decline in skeletal muscle mass and strength, affecting nearly one in three older adults. The process is multifactorial:
- Hormonal decline (testosterone, growth hormone, IGF-1)
- Decreased physical activity
- Chronic inflammation and illness
- Reduced protein intake and synthesis
This loss leads to
- greater risk of falls,
- frailty,
- functional dependence,
- and increased mortality.
Restoring muscle mass, therefore, remains a central therapeutic goal in geriatric medicine.
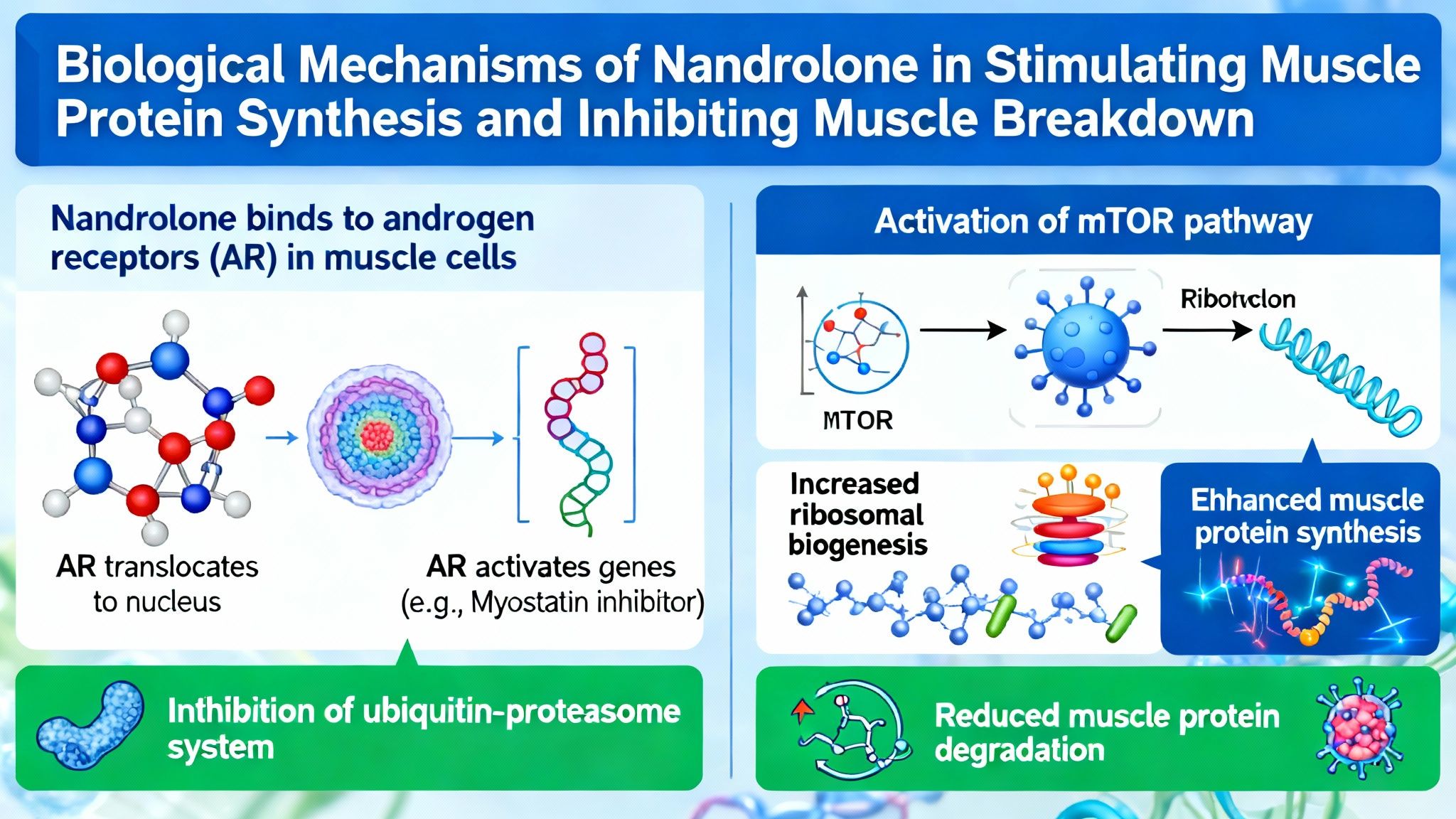
Mechanisms of Nandrolone—How Does It Work?
Nandrolone exerts its muscle-preserving actions via several interconnected pathways:
- Stimulates protein synthesis: Activates androgen receptors in muscle to enhance amino acid uptake and increase the building of new muscle protein.
- Inhibits protein breakdown: Blocks muscle protein degradation by suppressing catabolic pathways, including glucocorticoid-induced signaling.
- Boosts bone density: Increases bone mineralization through similar androgen receptor-mediated mechanisms.
- Modulates inflammation: Reduces pro-inflammatory cytokines, creating a more favorable environment for muscle maintenance.
These mechanisms explain why Nandrolone, in theory and in clinical studies, has shown promise for mitigating the muscle loss that accompanies aging and chronic disease.
Clinical Evidence for Nandrolone in Age-Related Muscle Wasting
Key Human Studies and Outcomes
Multiple clinical trials have evaluated Nandrolone in diverse populations, including elderly adults with sarcopenia, patients with chronic illness, and those with HIV/AIDS-related muscle wasting. The focus here is on its direct application to aging and sarcopenia.
Key Findings:
- Modest improvement in lean body mass: Several trials report meaningful increases in muscle mass, often 1–3 kg over 3–6 months, in older adults receiving Nandrolone.
- Strength improvements are variable: While some studies note better muscle strength and physical function, others observe gains in muscle mass without significant functional benefits.
- Best outcomes occur with exercise: The combination of Nandrolone therapy with resistance exercise produces superior results compared to either intervention alone.
- Impact on frailty is uncertain: Changes in quality of life, falls, and activities of daily living are inconsistent and require more study.
Efficacy for Specific Patient Groups
1. Elderly Adults with Sarcopenia
Nandrolone appears to provide a greater anabolic effect than testosterone in some cases, possibly due to its higher resistance to aromatization (conversion to estrogen). Short-to-medium term studies (12–24 weeks) consistently show increases in muscle mass compared to placebo.
2. Chronic Disease and Muscle Wasting
In populations with chronic kidney disease, HIV, or cancer, Nandrolone has helped maintain or increase muscle mass. Importantly, these uses are typically in the context of medically supervised, short-term courses.
3. Postmenopausal Women
Human research in postmenopausal women is limited but suggests similar trends—modest increases in lean body mass but concerns regarding virilizing side effects (voice deepening, hair growth).
Comparing Nandrolone to Other Approaches
Advantages
- Longer-acting than testosterone
- Lower risk of certain androgenic side effects
- Effective in both sexes (with caveats for women)
Limitations
- Anabolic effects are moderate in the elderly
- No replacement for exercise or nutrition
- Risks of long-term steroid exposure remain significant
Comparative studies versus SARMs (such as ligandrol or ostarine) are limited, but preliminary data suggest SARMs may offer a more favorable side effect profile with similar or slightly lower efficacy. [See also: Ligandrol LGD-4033 in Muscle Preservation].
Safety and Side Effects of Nandrolone
Common Side Effects
- Acne, oily skin
- Fluid retention
- Gynecomastia (male breast tissue growth), though lower risk than testosterone
- Voice changes, increased body hair (especially in women)
- Mood changes (irritability, aggression in some cases)
Serious Risks
- Suppression of natural testosterone production
- Cholesterol disturbances (lower HDL, higher LDL)
- Potential cardiovascular strain
- Liver enzyme changes (rarely severe at clinical doses)
- Prostate effects (benign enlargement, theoretical cancer risk)
Important Caution: Nandrolone should only be used under direct medical supervision and is not approved solely for age-related muscle loss in many regions. The safety profile is better established in short-term use for specific, medically indicated conditions.
Special Considerations for Aging Adults
- Higher sensitivity to cardiovascular and prostate effects
- Potential for impaired liver or kidney function
- Interactions with medications for common comorbidities
Practical Considerations for Nandrolone Therapy
Candidate Selection
Not all patients are appropriate candidates for Nandrolone. Consideration should be given to:
- Pre-existing cardiovascular, hepatic, or prostate disease
- Current medication profiles (statins, anticoagulants, anti-diabetic drugs)
- Baseline hormone and metabolic panels
- Lifestyle factors (diet, activity, alcohol use)
Dosing and Monitoring
- Typical clinical dosing: 50–100 mg intramuscularly every 2–3 weeks (varies by indication and patient)
- Monitoring: Lipid panel, hematocrit, liver/renal function, PSA (in men), blood pressure
Integrating With Lifestyle Approaches
Nandrolone is not a substitute for lifestyle interventions. Exercise (particularly resistance training) and optimal nutrition remain foundational.
| Intervention | Expected Impact |
|---|---|
| Nandrolone + Exercise | Largest muscle gain |
| Nandrolone alone | Moderate gain |
| Exercise alone | Moderate gain |
| Diet optimization | Preserves muscle |
Clinical pearl: In most studies, adding Nandrolone to a baseline regimen of exercise and nutrition optimizes muscle retention, but with diminishing returns compared to maximizing lifestyle first.
Common Questions About Nandrolone in Aging Populations
Is Nandrolone safe for treatment of sarcopenia?
Short-term, physician-supervised use appears reasonably safe in well-selected, closely monitored adults, but routine use for sarcopenia prevention is not currently recommended outside clinical trials due to long-term risks.
How does it compare to other anabolic therapies?
Nandrolone is more potent than testosterone esters in anabolic action, but also carries unique risks. Selective androgen receptor modulators (SARMs) may offer a safer alternative but are less well studied over the long term.
[Related: Ostarine MK-2866 for Age-Related Muscle Loss]

What are alternatives to steroid muscle therapy?
- Physical therapy and structured exercise programs
- Nutritional supplementation (e.g., high-protein diets, vitamin D, leucine)
- Selective androgen receptor modulators (SARMs)
- Peptide therapies under investigation
What is the outlook for anabolic steroid aging therapies?
Current medical consensus is cautious. Ongoing trials are clarifying:
- Who benefits most from such therapies
- Optimal dosing strategies to minimize risk
- Long-term effects on function, independence, and quality of life
The Research Context: Limitations and Gaps
While Nandrolone’s promise is clear in specific medical indications, several limitations affect its role in routine aging-related muscle therapy:
- Most studies short in duration (3–12 months)
- Blunted anabolic response in advanced age
- Risk-benefit ratio less favorable for long-term use
- Underrepresentation of older women in trials
Summary: Does Nandrolone Have a Role in Combating Age-Related Muscle Loss?
Nandrolone remains an effective anabolic steroid for select cases of muscle wasting related to aging or chronic illness. Human studies reveal modest, clinically relevant improvements in lean body mass and strength, especially in conjunction with exercise. However, its use for routine age-related muscle decline (sarcopenia) is limited by safety concerns and the lack of long-term data.
Nandrolone offers no substitute for exercise and nutrition, and should only be considered as part of a physician-directed, comprehensive plan. SARMs and other emerging therapies may ultimately address many of the shortcomings of steroid muscle therapy, but more research is needed.
Studies / References
- Effect on Muscle Mass & Bone Density in Elderly Women
- Frisoli et al. — Nandrolone decanoate increased lean body mass and bone density over 2 years in older women with osteoporosis.
https://pubmed.ncbi.nlm.nih.gov/15972619/
- Frisoli et al. — Nandrolone decanoate increased lean body mass and bone density over 2 years in older women with osteoporosis.
- Dose‑Finding Study in Chronic Kidney Disease
- Nandrolone increased appendicular lean mass in CKD patients; dose‑dependent increases noted.
https://pubmed.ncbi.nlm.nih.gov/17522475/
- Nandrolone increased appendicular lean mass in CKD patients; dose‑dependent increases noted.
- HIV‑Related Wasting (Multicenter RCT)
- Nandrolone decanoate increased weight and lean body mass in HIV‑infected women.
https://pubmed.ncbi.nlm.nih.gov/15767536/
- Nandrolone decanoate increased weight and lean body mass in HIV‑infected women.
- Hemodialysis + Resistance Training
- Combined nandrolone and resistance exercise produced additive increases in lean mass.
https://pubmed.ncbi.nlm.nih.gov/16825332/
- Combined nandrolone and resistance exercise produced additive increases in lean mass.
- HIV‑Infected Men (vs rhGH)
- Nandrolone increased lean body mass compared with placebo, similar to recombinant GH.
https://pubmed.ncbi.nlm.nih.gov/15914526/
- Nandrolone increased lean body mass compared with placebo, similar to recombinant GH.
Conclusion
For clinicians and patients contending with sarcopenia and muscle loss, Nandrolone is an evidence-based but limited tool. It can provide incremental gains in muscle mass when other modalities are insufficient, but evidence does not support widespread use due to significant safety considerations. A personalized, multidisciplinary approach—emphasizing exercise, nutrition, and careful consideration of pharmacotherapy—is paramount for healthy aging and muscle preservation.

